Tendon injuries are more recently know as tendonapathies. This is due to research that shows that there is little or no inflammation present at the injured site, unless there is an acute irritation. Tendonopathy is the failed healing of a tendon such as the achilles or forearm extensor and flexor tendons (tennis or golfers elbow) which occurs when breakdown exceeds repair.
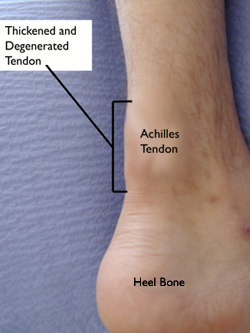
Healthy tendons are bright white and have a low blood supply or avascular with organised collagen fibres and work best in linear forces. Injured tendons, such as the achilles show disorganised or haphazard arrangement of the tendon cells (tenocytes) and collagen fibres. They also show neovascularization or an increase in blood vessels which have grown from deeper fibres and increased amount of proteoglycans which increases the water content of the tendon. The tendon become thickened, restricted and painful due to pain receptors (nocicepters) being irritated by the damaged tissue.

Chronic achilles tendinopathy
Tendons and inparticular the achilles tendon will withstand huge amounts of force and tension for long periods but chronic overload of the tendon will eventually lead to pain and injury as breakdown of the tissues exceeds healing and repair. The problem in managing a tendon injury is to get the rest/work balance right. Under working or sheilding the achilles, for example, will weaken the calf and associated muscles leading to cell changes and increasing the probability of further injury.
What leads to achilles injury?
- Over use
- Sudden increase in activity, intensity or length
- Degeneration due to under use
- Age, older/middle aged as weakened
- Lack of stretching leading to tight calfs
- Sudden stop/start ie re-starting after period of rest or intermittent high intensity activity
- Other factors are an increase in weigth and activity, flat feet, poor footwear.
Achilles problems usually start gradually with an ache at the beginning of activity ie running, then discomfort eases with movement but is stiff or tender after the activity. They are generally stiff and/or tender in the mornings and again eases with movement. The injury can be at the insertion into the back of the heel (calcaneum) or mid way up the tendon, as in the above photo. Scans have shown the achilles tendon to be much longer than we first thought with fibres extending almost up to the back of the knee. Considering this, the achilles must also be susceptible to injury higher up the calf too.
Management
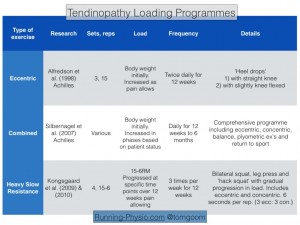
Most achilles tendonapathies are of a chronic nature without an inflammatory component so this programme will be structured for a chronic achilles tendonapathy. Injured tendon fibres need to be loaded in the direction of pull and they work most efficiently in a linear direction, infact injuries often occur when tendons are being stressed in a non-linear direction. Tendons adapt and strengthen or thicken normally when a reasonable load is applied to them.
- Calf stretching with knee straight and bent against the wall. Hold stretch for 15s and repeat.
- Isometric strengthening of the calf and achilles. Isometric is a static hold under tension. Go onto tiptoes of injured leg and hold for 10s building to 20 and 30s x 3. This can be progressed on a seated leg press machine to increase the load at your maximum for 8-12 reps x 3.
- Eccentric load. On a step use un-injured leg to go onto tip toes, lift that leg and place injured leg on tip toes and slowly lower to a count of 3, repeat 8-12 x 3. This exercise lengthens the achilles under tension whilst helping to stretch and realign the fibres.
- Combination of eccentric and concentric exercises. These can be added once the achilles has progressed. combine the above eccentric exercises with double then single leg calf raises. 8 reps x 3 of each. progress to a calf press on a leg press machine.
- Power training should be introduced once the achilles is fully pain free and if the patient is involved in sport ie running esp sprinting activities or jumping.
- Heat applied to the injured tendons will increase blood flow to the area and stimulate healing.

Alongside these rehabilitation exercises as an osteopath I would use manual soft tissue techniques to reduce tension in the calfs and friction to help break down and help realign the tendon fibres. Some joint manipulation of the foot and ankle may also be necessary to improve mechanics and kinesio taping to support or facilitae the achilles and calf muscles. Acupuncture and/or dry needling may also be included for pain relief and to reduce tension in trigger points within the calf.

Please feel free to leave a comment or ask any questions at the end of this blog. An appointment can be made with Lisa at Osteopath West by calling 07956 954093 or email lisa@osteopath-west.co.uk




